

Senescence and the Non-Pharmaceutical COVID-19 Work-Arounds
Senescence and the Non-Pharmaceutical COVID-19 Work-Arounds
The First of a Series of Related Posts
Introduction
Well, every cloud is said to have a silver lining, and there is a major one that seems to have emerged out of the whole COVID-19 hullabaloo. Willy-nilly, some of the human actions taken towards materially preventing or ameliorating the disease have helped to concretely confirm previous (‘before COVID19’) laboratory-level indications that a number of the major deleterious effects of aging are relatively easily halted and at least partially reversible.
COVID-19 mortality, like many other infectious and other diseases that can be fatal to people, is apparently strongly controlled by the age of the person concerned. See, for example, cumulative age-distribution of reported COVID-19 deaths in Minnesota in the graph below. Hardly anyone younger than the age of 301 has died because of COVID-19 in Minnesota (and elsewhere), but up to the age interval of 80-90, progressively increasing numbers of people/age interval do die from the virus. 2
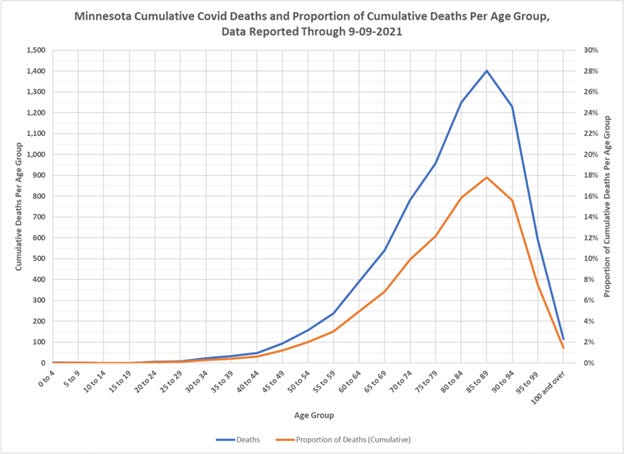
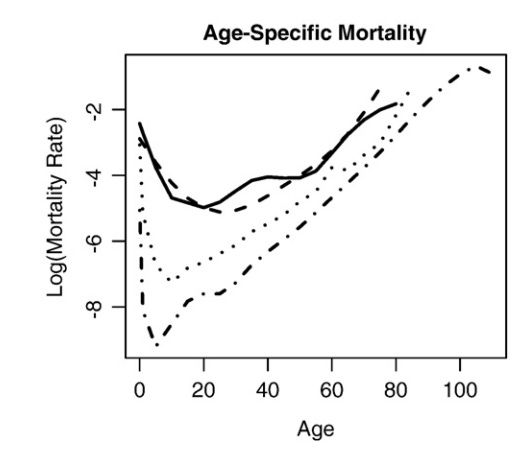
Note the strong correspondence between the above linear scale graph related specifically to COVID-19 and that log scale all-cause mortality graph provided below from Jones 2009. The dash-dot line in this second graph represents American population data.
Because not very many people even over the apparently critical inflection age point of 30 or so years (again, graphs above), permanently succumb to the virus, however, it is clear that increasing age is not an absolute predictor of death by COVID-19. There are many confounding variables: age is therefore only generally related to another more tangible and mortality-predictive human biological characteristic, senescence. As first formally defined by the biologist, P.B. Medawar, the distinction between aging and senescence is this:
We obviously need a word for mere aging, and I propose to use 'aging' itself for just that purpose. 'Aging' hereafter stands for mere aging, and has no other innuendo. I shall use the word 'senescence' to mean aging accompanied by that decline of bodily faculties and sensibilities and energies which aging colloquially entails.
Because not all people develop the “…decline of bodily faculties and sensibilities and energies” at the same rate and to the same degree with their increasing age, not all people of a given age are equally at risk for death from the various diseases that afflict human lives. This includes the cardiovascular and inflammatory diseases like those potentially engendered by exposures to the COVID19 virus.
So?
Very, very interestingly, all of the various oral supplements and/or non-vaccine medicines shown to substantially decrease infection and mortality rates associated with bacterial and viral respiratory illnesses – including COVID19 -- appear to work by materially renovating major biochemical/biological systems affected by human senescence, including those systems governing immunity to pathogens like respiratory viruses.
To date, the list of readily available preventive or prophylactic substances3 found to be significantly protective against respiratory viruses (and bacteria) including COVID-19 is this:
Zinc
Various zinc ionophores
Vitamin D3
Arginine and citrulline (both are nitric oxide precursors)
N-Acetyl Cysteine (“NAC” is a glutathione precursor)
NAD+ precursors like niacin
Contrasting Areas of Operation of Prophylactics/Preventives vs. Vaccines
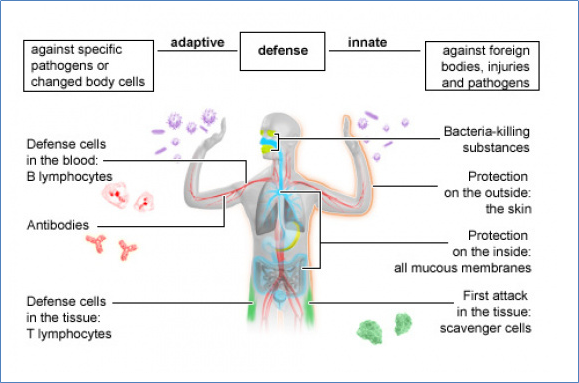
The first or front line of defense against bacterial or viral infection is the innate immune system, while the second or ‘last-ditch’ line of defense is the adaptive immune system.4 See diagram below and ibid. (footnote 4) for more detail. The innate immune system works to stop or minimize the initial, local entry of foreign invaders into the body. On the other hand, the adaptive immune system seizes upon pathogens escaping past the first-line innate immune system to tailor pathogen-specific defenses against such especially problematic viruses and microorganisms that can potentially cause systemic infections like those seen in people with severe COVID-19 infections whose poorly-functioning innate immune systems failed to minimize COVID19 cellular entry and subsequent viral replication.5
As the references provided in later posts addressing the basic research initially supporting the use of each preventive/prophylactic show, the six different substances listed above have long6 been determined to support the function of both the innate and adaptive immune systems. The various COVID-19 vaccines, on the other hand, support only the function of the adaptive (the ‘last-ditch’) immune system, and do nothing to prevent the original entry of COVID-19 into human cells. Generally speaking, the preventives and prophylactics address deficiencies in substances that are important to enzyme, cell-signaling, and hormonal systems that gradually appear over time (i.e., during increasing senescence) because of poor nutrition, declining physical activity (especially outdoors), and increased cellular demands and other disturbances caused by incremental development of vicious cycle/positive feedback loops.
There’s a dominant hypothesis in evolutionary theory that natural selection doesn’t much ‘care’ what happens to humans after they’ve reproduced and their children have themselves reached reproductive age. See https://en.wikipedia.org/wiki/George_Christopher_Williams and https://www.science.org/doi/epdf/10.1126/sageke.2001.1.cp13. This hypothesis in fact suggests genetic traits supportive of youthful reproduction can actually cause later senescence.
In Minnesota and elsewhere, after the age of 80-90 there are fewer and fewer people in the Minnesota population still alive to contract the disease and die. Thus, the observed drop in the number and proportion of deaths after that highest incidence age interval.
https://www.merriam-webster.com/dictionary/prophylactic For a summary description of the practical use of most of these substances, see https://swprs.org/on-the-treatment-of-covid-19/.
https://www.ncbi.nlm.nih.gov/books/NBK279396/
https://www.healthtap.com/questions/194985-what-is-a-systemic-infection/. COVID-19 secures entry to human cells through ACE2 receptor sites found on the surface of human cells. Interestingly, children have far fewer ACE2 receptor sites on their cell surfaces, so apparently have greater innate immunity to COVID-19 viruses and are therefore far less likely to develop acute systemic infections of the virus. Note that increasing senescence is always marked by decreasing functionality of the innate and adaptive immune systems.
Decades before ‘the COVID’ and the controversial 2020 Zelenko Protocol.